Syncope
Syncope
Definition
Syncope (commonly called fainting) is a temporary loss of consciousness and muscle tone caused by a brief reduction of blood flow to the brain. It usually starts suddenly, lasts for a short time (seconds to minutes), and is followed by a quick and complete recovery. Syncope is a symptom, not a disease. It can occur in healthy people or be a sign of an underlying heart or autonomic nervous system problem.
Why does syncope occur?
The brain needs a constant supply of oxygen and nutrients. If blood flow suddenly decreases, even for a few seconds, you can lose consciousness. This can happen because of:
- A drop in blood pressure (vasodilation which means that your blood vessels widen or relax, allowing more blood to flow through them), dehydration, standing too long)
- A sudden drop in heart rate
- Irregular, rapid or slow heart rhythms (heart rhythm disorders, so called arrhythmias)
- Structural heart disease that limits blood flow (for example a narrowed heart valve or heart failure)
Main types of syncope
| Type | Mechanism / Cause | Common Triggers | Typical Clues |
| Reflex (Neurally Mediated) Syncope
(Vasovagal syncope is the most frequent reflex syncope) |
Overreaction of the autonomic nervous system* → sudden drop in heart rate and blood pressure | Emotional stress, pain, sight of blood, prolonged standing | Nausea, sweating, ‘tunnel vision’ before fainting |
| Orthostatic Hypotension | Blood pressure falls when standing up | Dehydration, hot weather, blood loss, possibly prescribed drugs | Fainting soon after standing, especially in the morning |
| Cardiac Syncope | Due to heart rhythm problems or structural heart disease | Heart rhythm disorder (Arrhythmia), heart block, aortic stenosis (narrowed valve in the heart and because the opening of the valve is smaller, the heart has to work much harder to push blood through it, pacemaker malfunction (it is not working the way it should) | Often sudden, without warning; may occur during exertion |
| Other / Non-syncopal Causes | Not true syncope, but can mimic it | Seizures, low blood sugar, anxiety (psychogenic pseudo-syncope), vertigo | Symptoms are usually different from syncope |
* The autonomic nervous system is the part of your nerves that works automatically without you having to think about it. It controls things like your heart rate, blood pressure, breathing, digestion, and sweating.
What are the symptoms?
Before fainting, many people experience warning signs also called prodromes, including:
- feeling weak
- nausea
- cold sweating
- blurred vision or “dark spots”
- ringing in the ears
- feeling warm or light‑headed
- palpitations (Palpitationsare the feeling that your heart is beating in an unusual way. You might notice it racing, skipping beats, fluttering, or pounding harder than normal)
After falling, recovery is usually quick, although some people may feel confused or tired for a short time.
Which tests help identify the cause?
The evaluation is done step by step, starting with the simplest tests:
- Medical Visit and Symptom Review
Your doctor will talk with you about what happened, whether you felt any warning signs before you fainted, what you were doing at the time, and any medical conditions or medications you have. This conversation is often the most important step in finding the cause.
Your blood pressure will also be measured both lying down and standing to see how your body reacts to position changes.
- Electrocardiogram (ECG)
A quick, painless test that records heart activity. It helps detect heart rhythm disorders (arrhythmias) or other heart problems.
- Tilt Table Test (sometimes performed)
The tilt table test helps determine whether the syncope is vasovagal or orthostatic. During the test, the patient lies on a special table and is safely strapped in. At first, the table stays flat while heart rate and blood pressure are checked. Then the table is slowly tilted upright, as if the patient were standing. While in this position, the doctor observes how the body reacts. The test helps show whether the symptoms are caused by a drop in blood pressure or a change in heart rate.
Carotid sinus massage (massage of the carotid artery at the level of the neck) may be performed at the same time to trigger a reflex syncope.
- 24-hour blood pressure monitoring (sometimes performed)
A small, portable blood-pressure recorder will be worn for a full day and night. The device automatically takes blood pressure at regular intervals (usually every 15–30 minutes) during the day and every 30–60 minutes at night. Low blood pressure suggests either orthostatic hypotension or a reflex (vasovagal) syncope.
- Blood Tests (sometimes performed)
Blood tests are used to check for anemia, blood sugar levels, electrolytes, and possible dehydration.
- Echocardiogram (sometimes performed)
An ultrasound test used to evaluate the heart’s structure and valves. Recommended when a cardiac cause of the syncope is suspected.
- Long term ECG monitoring recorder (sometimes performed)
Holter monitoring is sometimes performed. A small device is worn for 24–72 hours (or longer) to record heart rhythm. Useful when arrhythmia‑related syncope is suspected.
In case of syncope, 24-72 hours of ECG monitoring may be insufficient. In this situation, an implantable loop recorder may be implanted: it is a very small device placed under the skin of the chest. It continuously monitors your heart rhythm for many months. It helps doctors find the cause of symptoms like fainting, dizziness, or palpitations when regular tests do not give an answer.
Treatment
The treatment of syncope focuses on identifying and addressing the mechanisms that lead to a temporary drop in blood flow to the brain. Management is personalized, depending on whether the cause is related to blood pressure regulation, heart rhythm abnormalities, or structural heart disease. Common treatment strategies include:
- Lifestyle and preventive measures for reflex or vasovagal syncope
Many patients benefit from simple strategies such as staying well hydrated, avoiding long periods of standing, and recognizing early warning signs like dizziness, nausea, or blurred vision. When these symptoms appear, lying down or performing physical counter-pressure maneuvers (like crossing the legs or tensing the leg and abdominal muscles) can help raise blood pressure and prevent a fainting episode (figure 1).
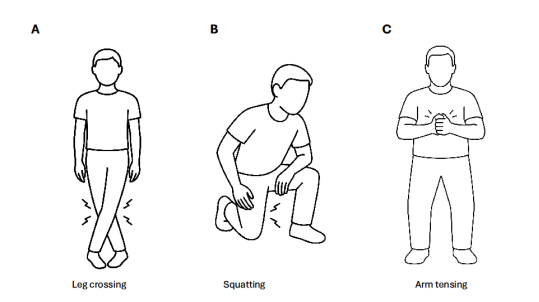
Figure 1. Counter-pressure maneuvers
- Treatment of heart rhythm disorders
If syncope is caused by an abnormal heart rhythm, therapy is targeted to correct the arrhythmia.
- Pacemakers may be recommended when the heart beats too slowly or pauses.
- Implantable defibrillators (ICDs) are used when fainting is related to dangerous fast rhythms.
- Catheter ablation can be used to eliminate certain rhythm problems that trigger syncope.
- Deprescription:
Since many medications can induce orthostatic hypotension, the management of reflex or orthostatic hypotension syncope often involves deprescribing these agents. This includes reducing or discontinuing antihypertensive medications or treatments for anxiety, depression, or urinary symptoms related to prostate conditions. Any changes to medications should be discussed in detail with the treating physician to ensure safety and appropriateness.
- Cardioneuroablation
In some cases, for patients with recurrent reflex (vasovagal) syncope driven by an excessive vagal response causing marked slowing of the heart rate (significant bradycardia or even pauses/asystole), a specialized procedure called cardioneuroablation may be considered.
This invasive treatment uses catheter ablation to modify specific nerve clusters in the heart that are responsible for exaggerated vagal responses. For this procedure, the heart is accessed via the groin. The goal is to reduce the frequency and severity of fainting episodes when other treatments have not been effective.
- Medications
In selected cases, medicines may be used to help stabilize blood pressure, reduce excessive vagal responses, or manage associated rhythm disturbances. These are tailored to the individual and are not needed for all patients.
- Managing underlying cardiovascular conditions
Treating contributing factors such as structural heart disease, anemia, dehydration, or blood pressure instability can help prevent future episodes.
Overall, most patients experience significant improvement when therapy is adapted to the specific cause of their syncope. Cardiologists and electrophysiologists work together to determine the most effective and safest treatment plan for each patient.